Learning Materials

Reproductive Immunology 101
Reproductive Immunology is a very important yet poorly understood field which affects fertility and pregnancy outcomes. While great progress has been made in applying immunology treatments to fight cancer, improve organ transplant survival, and treat autoimmune disorders, relatively little progress has been made in reproductive medicine. One of the most important recent discoveries in reproductive immune medicine was the identification of HPV virus as the cause of cervical (and other) cancers and subsequent development of HPV vaccines.
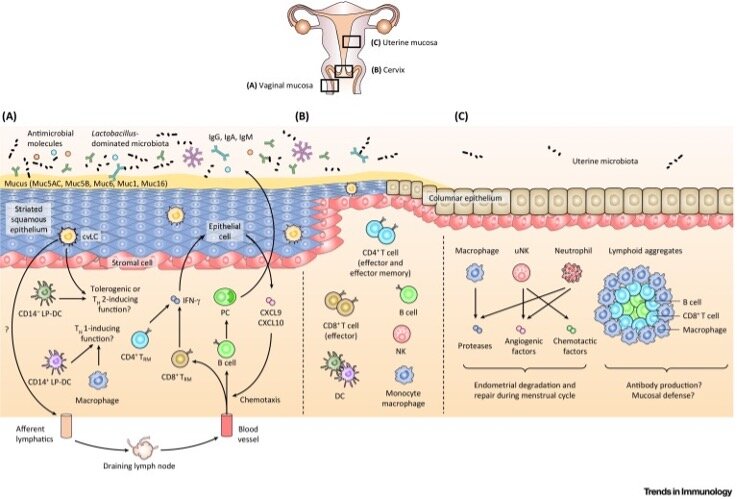
Healthy endocrine and immune systems work closely together to enable reproduction while providing immune protection against sexually transmitted infections (STI). Hormonal changes during the menstrual cycle affect the distribution and function of immune cells in the female reproductive tract. For example, estrogen and progesterone hormones affect immune cells in the endometrium to prevent sperm rejection and to prepare the endometrium for implantation of the embryo. In order to create this implantation window for the embryo the immune and endocrine systems inadvertently also create a window of vulnerability during the secretory phase of the menstrual cycle during which the reproductive tract is more susceptible to infections.
Similarly, fluctuation in corticotropin-releasing hormone (CRH) which regulates the stress response predispose women to windows of vulnerability to mood disturbances and autoimmune disorders during key transitions in life including puberty, early menopause, immediately postpartum, and just prior to menstruation (PMS).
Normal ovulation and menstruation trigger cyclic tissue remodeling. The endocrine and immune systems direct activation of blood coagulation and remodeling of local blood vessels. Abnormal inflammation which can be related to infection or an exaggerated immune response contributes to common reproductive disorders including endometriosis, infertility and pregnancy complications.
Anti-inflammatory drugs and drugs that interfere with cyclic tissue remodeling are often used to treat reproductive disorders. Examples include nonsteroidal anti-inflammatory (NSAID) drugs like ibuprofen, steroids like dexamethasone, antibiotics in cases of infection, and hormonal contraceptives which interrupt cyclic tissue remodeling.
Zhou JZ, et al. Trends Immunol. 2018 Apr;39(4):302-314.
Maternal Immune Tolerance of Pregnancy
The maternal immune system interacts with the growing fetus and placenta via a process of alloimmune recognition followed by induced tolerance. Because the fetus expresses paternal antigens it is foreign to the mother, yet a healthy maternal immune system is able to tolerate the pregnancy for 9 month. One consequence of this relative immune suppression during pregnancy is that women at increased susceptibility to infections some of which can also be more severe during pregnancy.
It has been proposed that many pregnancy related disorders including recurrent embryo implantation failure, miscarriage, preterm labor and preeclampsia are related to abnormal induction of tolerance. Though it’s not completely understood how immune tolerance to pregnancy is induced, there is convincing data that exposure to paternal antigens in semen prior to pregnancy allows the maternal immune system to develop tolerance by activation of maternal Treg cells. Exposure to semen has been associated with a reduction in some pregnancy disorders, improved fetal development, and improved IVF pregnancy rates.
Genest, F&S Reviews 2022 324-41G.
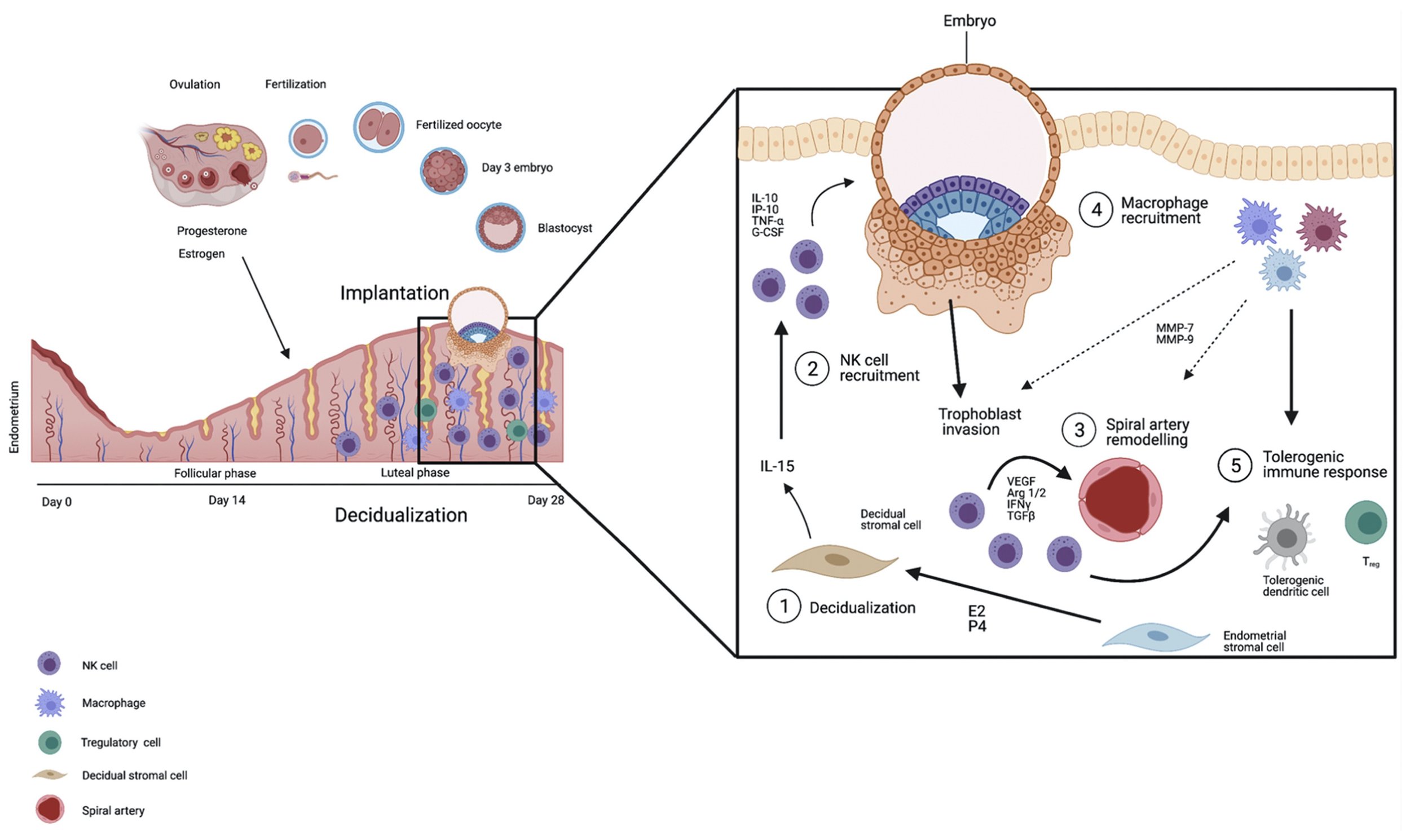
This diagram shows that at time of embryo implantation immune cells in the uterus constitute 40% of the total decidual cell population. The most common cells responsible for innate immunity are decidual natural killer cells, macrophages, dendritic cells and T-lymphocytes. It has recently been recognized that natural killer cells (NK) are very important in promoting fetal development because they secrete growth promoting factors. During later stages of pregnancy circulating maternal immune cells interact with the growing placenta. Thus, during late pregnancy systemic rather than local immune responses become more pronounced.
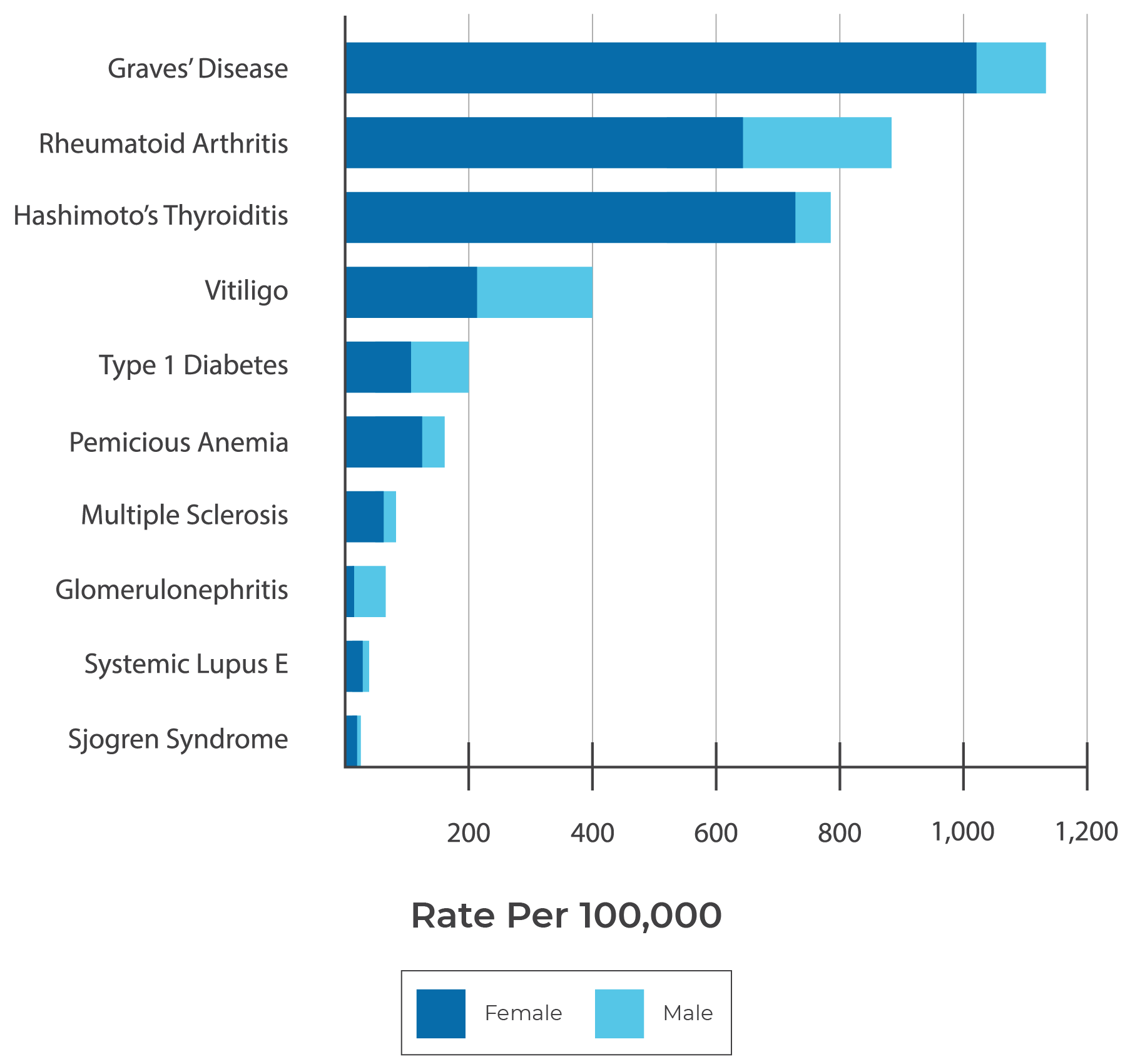
Women with autoimmune disorders like thyroiditis, lupus and rheumatoid arthritis have significantly increased risk for serious complications during pregnancy. Additionally, many autoimmune disorders can flare shortly after delivery while some flare during pregnancy. Autoimmune disorders disproportionately affect women especially during the childbearing years. This is at least partially related to high prevalence of immune genes which are found on the X chromosome and to hormonal changes during these years. Even women who do not have a clinically diagnosed autoimmune disease but only have subclinical autoimmunity due to presence autoantibodies and those with abnormal inflammation are at increased risk for pregnancy complication.
Antiphospholipid antibody syndrome (APS) is one of the most well understood autoimmune disorders which causes miscarriages, stillbirth, premature birth and severe preeclampsia. APS is due to autoantibodies that cause blood clots, these clots can also cause strokes, pulmonary embolism and deep vein thrombosis. APS is treated with anticoagulants like aspirin and heparin which prevent blood clots.
Pregnant women who have Lupus are often treated with medications like Plaquenil (hydroxychloroquine) and Prednisone. Prednisone is metabolized by the placenta, and is unlikely to cause fetal malformations, but increases the risk of diabetes and hypertension in the mother. In some cases immunosuppressive drugs like imuran (azathioprine) are also used during pregnancy. Cyclophosphamide, ACE-inhibitors and Coumadin cause birth defects and have to be stopped. Heparin can be used during pregnancy to prevent bloodclots. NSAIDs are usually only used during the first trimester.
Hashimoto’s and Graves are autoimmune disorders affect the thyroid gland. Both are due to autoantibodies which affect the function of the thyroid gland. Women with Hashimoto’s have hypothyroidism and are treated with thyroid hormone, this is especially important during pregnancy since fetal brain development depends on getting adequate thyroid hormone from the mother. In Graves disease autoantibodies cause hyperthyroidism, treatment includes drugs like PTU and methimazole.
Rheumatoid Arthritis usually improves during pregnancy but can flare after delivery; risks of pregnancy related complications are only slightly increased. Low-dose Prednisone, Plaquenil and Sulfasalazine are generally considered safe during pregnancy. There is only limited evidence about safety of biologic medicines like etanercept (Enbrel), infliximab (Remicade), and infliximab-abda (Renflexis), still many rheumatologists advise patients to continue these drugs during pregnancy.
Diagram: Prevalence of Autoimmune Diseases
Reproductive Immune Evaluation:
The reproductive immune evaluation is guided by the couple’s medical history. It may involve blood tests to look for autoimmunity and systemic inflammation, hormone levels, and an endometrial biopsy to evaluate for chronic endometritis which is due to local inflammation and/or infection inside the uterus. In some cases, a hysteroscopy may also be indicated to closely evaluate the endometrium for inflammation.
Reproductive Immune Treatments (A to Z)

Genest, F&S Reviews 2022 324-41G.
For patients with diagnosed autoimmune disorders there are widely accepted treatment strategies for prior to and during pregnancy. However, for patients with subclinical autoimmunity and inflammation there is less clarity. Because of the heterogeneous presentation of patient with these conditions very few high-quality clinical studies exist, thus there is a lack of scientific evidence upon which treatment strategies can be developed.
For infertile patients and those with history of recurrent miscarriage who do not have an underlying autoimmune disease, suppressing the maternal immune system with medications has for the most part not been successful in improving implantation or preventing miscarriage. The current focus in reproductive immunology has shifted away from therapies aimed to suppress the maternal immune system in favor of those intended to enhance tolerance of paternal antigens and of the fetus.
Below is a partial list of reproductive immune medications and treatments, though the level of evidence behind most of these is often limited and therefore may not be appropriate for most patients with fertility and pregnancy issues. It is also important to recognize that many medications, especially hormones, used in fertility treatment have secondary effects on the immune system.
Adalimumab (Humira) – is a tumor necrosis factor alpha (TNFa) blocking antibody used to treat autoimmune conditions including psoriasis, rheumatoid arthritis, psoriatic arthritis, and inflammatory bowl diseases (IBD) this medication is generally considered safe to use during pregnancy.
Aspirin – Is a nonsteroidal anti-inflammatory drug (NSAID) which also has blood thinning properties, it is used for patients with history of recurrent pregnancy loss, clotting disorders and preeclampsia. Aspirin is frequently used to reduce fever, pain and swelling.
Azathioprine (Imuran) – suppresses the immune system by interfering with DNA synthesis. It is used in many autoimmune and inflammatory disorders. There is evidence of fetal risk but potential benefits may warrant use of this drug in some pregnant women.
Cyclosporine – is an immunosuppressive drug used to prevent organ rejection after transplant and for some autoimmune conditions including psoriasis and rheumatoid arthritis. During pregnancy there is no increased rate of birth defects, but low birth weight and premature birth have been linked to cyclosporine use. Cyclosporine should only be used during pregnancy if the benefits outweigh the potential risks.
Dehydroepiandrosterone (DHEA) – is a natural hormone produced by the adrenal gland. DHEA is converted to other hormones including testosterone and estrogen. Natural DHEA levels peak in early adulthood and then slowly falls with age. DHEA is often used to counter effects of aging and in fertility treatments for women with low androgen levels. DHEA supplementation has been shown to activate the immune system.
Dexamethasone – is a long-acting corticosteroid medication with anti-inflammatory and immunosuppressive properties. It is useful for a variety of immune disorders and can be used during pregnancy to help mature fetal lungs. Dexamethasone is also used to lower androgen levels in PCOS patients during ovulation induction.
Doxycycline – is an antibiotic with anti-inflammatory properties. It is often used to treat or prevent infections in the reproductive tract.
Enoxaparin sodium (Lovenox) – is a Low-molecular-weight heparin (LMWH) decreases the clotting ability of blood and can prevent harmful clots from forming in blood vessels. It can help prevent miscarriage in patients with antiphospholipid antibody syndrome (APS), it can also be used to prevent preeclampsia and fetal growth restriction. Lovenox does not cross the placenta and is generally considered safe to use during pregnancy.
Estradiol – is the main estrogen hormone in premenopausal women, it affects virtually all cells in the immune system. Estrogen has been shown to have different effects in various autoimmune diseases, some improve while others worsen.
Glatiramer acetate (Copaxone) – is used for treatment of multiple sclerosis it stimulates the production of myelin and suppresses the immune system by preventing T-cells from damaging myelin. Copaxone seems safe to use during pregnancy.
Granulocyte Colony-Stimulating Factor (G-CSF) – is a glycoprotein that stimulates the bone marrow to produce granulocytes and stem cells and release them into the bloodstream. It is mostly used in patients with chemotherapy induced neutropenia, and during stem cell transplantation and before blood donation. Studies of G-CSF to prevent miscarriage and in conjunction with infertility treatment have produced divergent results.
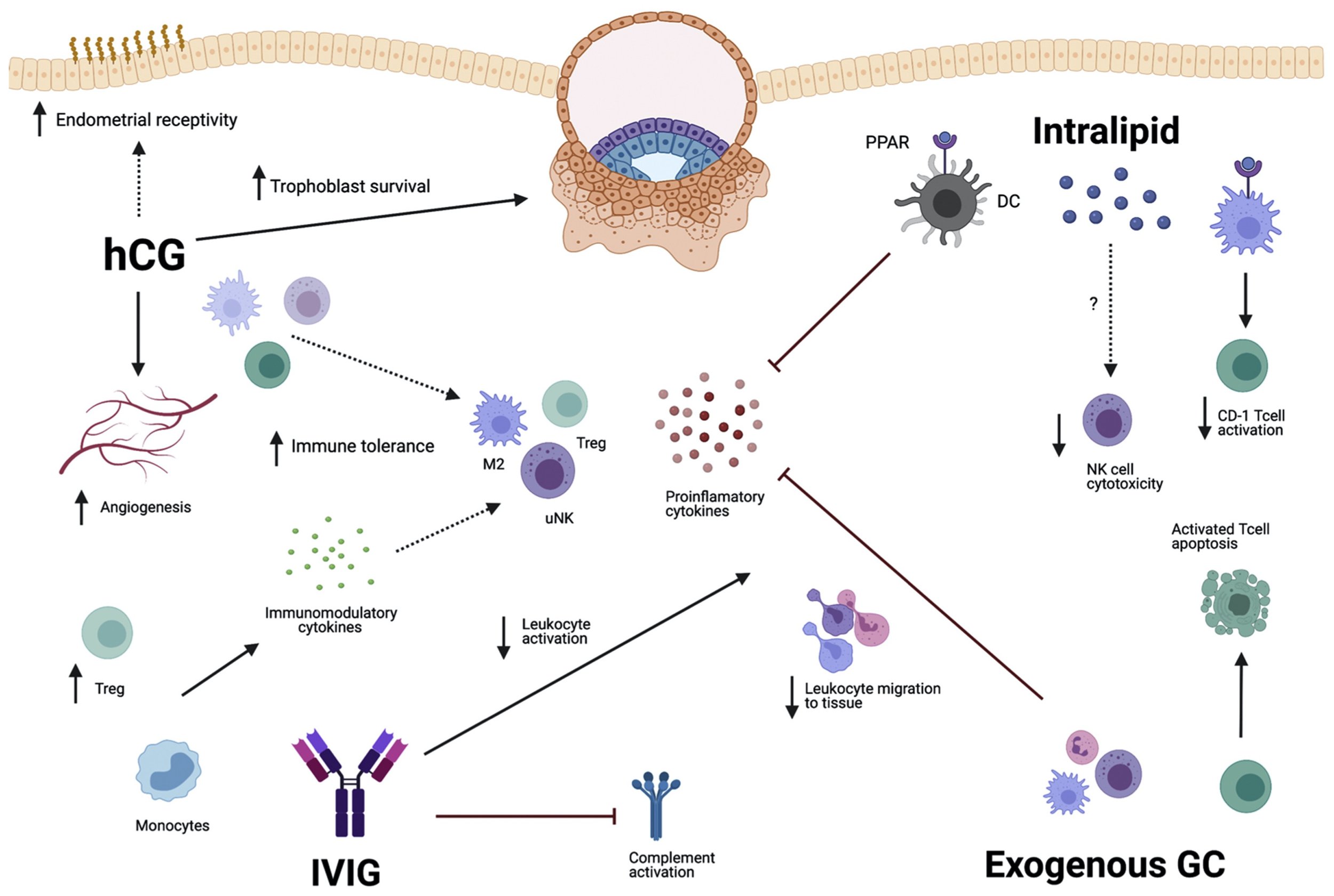
Human Chorionic Gonadotropin (HCG) – is one of the main pregnancy hormones which is involved in implantation and placentation. HCG regulates the maternal immune system allowing the tolerance of foreign fetal antigens. HCG is often given during fertility treatments to induce ovulation, maintain the corpus luteum and sometimes during early pregnancy.
Human Growth Hormone (HGH) – is used to treat HGH deficiency and occasionally to improve oocyte quality in patients with severe diminished ovarian reserve. HGH has a variety of effects on the immune system, especially on differentiation of T cells in the thymus gland.
Heparin – is an injectable anticoagulant. Heparin decreases the clotting ability of blood and can prevent harmful clots from forming in blood vessels. It can help prevent miscarriage in patients with antiphospholipid antibody syndrome (APS), it can also be used to prevent preeclampsia and fetal growth restriction.
Hydroxychloroquine (Plaquenil) – is a medication used to treat malaria and autoimmune conditions including rheumatoid arthritis and lupus. Plaquenil is frequently used to treat these autoimmune disorders during pregnancy thought it is thought it is associated with a low risk of eye and ear anomalies.
Ibuprofen – is found in many of over-the-counter medicines. It is a non-steroidal anti-inflammatory drug (NSAID) used to treat pain, inflammation and fever. Ibuprofen should be avoided during pregnancy due to increased risk of miscarriage and around the time of ovulation by women who are trying to conceive
Infliximab (Remicade) – blocks tumor necrosis factor alpha, decreases inflammation and the immune response. It is used to treat many autoimmune disorders including arthritis and inflammatory bowel diseases (IBD). Though infliximab crosses the placenta it is generally considered safe to use in pregnancy.
Intralipid – is a synthetic product composed of soybean oil, egg yolk phospholipids, glycerin, and water. Intralipid is thought to suppresses natural killer (NK) cell cytotoxicity. Currently data is lacking to show positive effects on fertility with Intralipid, though it has a favorable safety profile.
Intravenous Immunoglobulin (IVIG) – is a blood product prepared from the pooled serum of many donors, it has immune-modulating and anti-inflammatory properties. IVIG is used to treat an increasing number of immune and inflammatory disorders. A number of small studies have been conducted in patients with infertility and recurrent pregnancy loss, some showed improvement in implantation rates and live birth rates while other studies found no benefit.
Interferon beta – is a cytokine used to treat multiple sclerosis. While no birth defects have been identified during pregnancy this medication has been linked to increased risk of miscarriage. Risk of relapse following discontinuation of this drug during pregnancy should be weighed against a possible increased risk of miscarriage.
Lymphocyte Immunization Therapy (LIT) – is a procedure where white blood cells from the male partner are injected into the skin of the female with the intention to induce tolerance of paternal antigens by the maternal immune system prior to pregnancy. This procedure is not permitted in the United States due to safety concerns.
Metformin (Glucophage) – decreases liver glucose production, intestinal glucose absorption and increases target cell insulin sensitivity. It also influences gut microbiota and the immune system. Metformin is used to treat diabetes prior to and during pregnancy. It can be helpful in women with insulin resistance and PCOS to improve fertility and pregnancy outcomes.
6-mercaptopurine (6-MP, Purinethol) – suppresses the immune system by interfering with DNA synthesis. It is used in inflammatory bowel disorders and as a chemotherapy drug. This drug can cause fetal harm, but potential benefits may warrant use of this drug in some pregnant women.
Naltrexone – is an antagonist for opiate/endorphin receptors, it is mostly used for patients fighting narcotic and alcohol dependence. When used in low doses naltrexone (LDN) acts an immunomodulator. Fertility effects of naltrexone have not been systematically studied in humans.
Naproxen – is found in many of over-the-counter medicines. It is a non-steroidal anti-inflammatory drug (NSAID) used to treat pain, inflammation and fever. Naproxen should be avoided during pregnancy due to increased risk of miscarriage and around the time of ovulation by women who are trying to conceive.
Omega 3 Fish Oil – essential fatty acids that must be consumed in the diet. The two most biologically active omega-3s are EPA and DHA. EPA supports the heart, immune system, and inflammatory response while DHA supports the brain and eye development. These fatty acids are often added to prenatal vitamins.
Peripheral blood mononuclear cells (PBMCs) – Intrauterine infusion of PBMCs has been studied with the intention to overcome repeated implantation failure by modulating the intrauterine immune environment. While improvement in clinical pregnancy rates have been shown in some studies, so far improvement in live birth and miscarriage rates have not been established.
Platelet Rich Plasma (PRP) – injection of PRP into the ovaries and uterus are under investigation to determine whether it can ‘regenerate’ these organs. Research is aimed to see whether cytokines and growth factors in PRP can activate ovaries or recruit stem cells to the endometrium to improve function of these tissues.
Pravastatin – is used to lower cholesterol and triglycerides in the blood and slow down atherosclerosis (hardening of the arteries). Recently it was discovered that pravastatin may reverse pathophysiology of preeclampsia including angiogenic imbalance, endothelial injury, inflammation, and oxidative stress. It is now studied in clinical trials to prevent preeclampsia. Pravastatin is a water-soluble statin and has a favorable safety profile in pregnancy.
Prednisone – is a short-acting corticosteroid medication with anti-inflammatory and immunosuppressive properties. It is useful for a variety of immune disorders and can be used during pregnancy since it is inactivated by the placenta.
Pre-Implantation Factor (PIF) – is a naturally occurring peptide secreted by embryos. PIF has immune-modulatory effects and is currently undergoing clinical trials in pregnancy, autoimmunity and transplant fields.
Progesterone – is one of the main hormones of pregnancy it also has significant immunological properties. Progesterone is often started after ovulation to support embryo implantation and subsequent pregnancy. It is also used to decrease risk of premature birth. Progesterone induces a Th2 dominant cytokine environment and concurrently suppresses inflammatory immune responses.
Rituximab (Rituxan) – is a chimeric monoclonal antibody which binds to the surface of B cells. It is used for treatment of several autoimmune diseases and lymphoma. This drug should be used during pregnancy only if the benefit outweighs the risk.
Seminal plasma – refers to the components of human semen other than sperm cells. Seminal plasma contains proteins that interact with cervical and uterine epithelial cells inducing active immune tolerance. A number of studies showed that women undergoing IVF who were exposed to seminal plasma around the time of egg retrieval or embryo transfer, achieved higher clinical pregnancy but not live birth rates.
Sirolimus (Rapamune) – is an mTOR inhibitor with potent immunosuppressive effects, it is used in organ transplantation. It is currently under investigation for treatment of women with recurrent implantation failure.
Sulfasalazine (Azulfidine) – is a sulfa drug used to treat rheumatoid arthritis, inflammatory bowel disease, and other autoimmune conditions. It is often used during pregnancy to prevent a flare-up of these immune disorders. Because sulfasalazine lowers folic acid levels, women should be taking 5 mg of folic acid daily.
Tacrolimus (Prograf) – is an immunosuppressive drug used to prevent solid organ rejection in transplant patients. There is limited evidence for tacrolimus in patients with recurrent implantation failure and recurrent pregnancy loss who have elevated Th1/Th2 cell ratios
Vitamins & Minerals – have multiple effects on reproductive and immune systems. It is advised that women obtain vitamins and minerals primary from diet and avoid both deficiency and excess intake. Women are advised to take a prenatal vitamin while trying to conceive and during pregnancy.
Vitamins: A, B6, B9 (folate) B12, C, D, E, K
Calcium, Magnesium, Iron, Selenium, Zinc
Some immune drugs including Methotrexate, Cyclophosphamide, Thalidomide and Retinoids should always be avoided during pregnancy due to high risk of birth defects.
